.
The lead article in the New York Times (right column, front page, by Annie Lowrey and Robert Pear) on Sunday, July 29, 2012, has the provocative headline “Doctor shortage likely to worsen with health law.” My first instinctive reaction was “What? I don’t know of any part of the new health law, the ACA, that will reduce the number of doctors!” Then, reading the first sub-head, I realized what they meant. “Primary care is scarce”, something I well know and have written a lot about, and then, in smaller type, “Expanded coverage, but a greater strain on a burdened system.”
The lead article in the New York Times (right column, front page, by Annie Lowrey and Robert Pear) on Sunday, July 29, 2012, has the provocative headline “Doctor shortage likely to worsen with health law.” My first instinctive reaction was “What? I don’t know of any part of the new health law, the ACA, that will reduce the number of doctors!” Then, reading the first sub-head, I realized what they meant. “Primary care is scarce”, something I well know and have written a lot about, and then, in smaller type, “Expanded coverage, but a greater strain on a burdened system.”
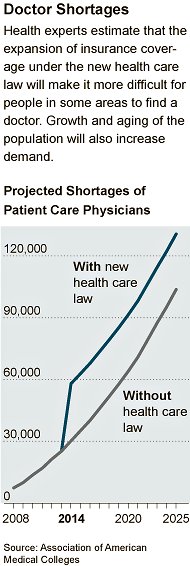 What they are saying is that the shortage of physicians, especially primary care physicians, will effectively increase (get worse) as millions more people gain insurance coverage under ACA. This will happen both through expansion of Medicaid coverage or through health insurance exchanges that will permit both individuals and small companies that have not previously had or offered health insurance to buy it at much lower rates. The expansion of health insurance coverage to these groups is a good thing; it will eliminate a major barrier to quality health care, itself a component of good health. Unfortunately, phrasing the problem in the way that the NYT headline does is likely to inflame displeasure with the law among those who, through ignorance or selfishness or both, are happy to draw up the bridge behind themselves, not wishing to share their, often limited, access to doctors with the newly insured. Surely, this is not an acceptable reaction.
What they are saying is that the shortage of physicians, especially primary care physicians, will effectively increase (get worse) as millions more people gain insurance coverage under ACA. This will happen both through expansion of Medicaid coverage or through health insurance exchanges that will permit both individuals and small companies that have not previously had or offered health insurance to buy it at much lower rates. The expansion of health insurance coverage to these groups is a good thing; it will eliminate a major barrier to quality health care, itself a component of good health. Unfortunately, phrasing the problem in the way that the NYT headline does is likely to inflame displeasure with the law among those who, through ignorance or selfishness or both, are happy to draw up the bridge behind themselves, not wishing to share their, often limited, access to doctors with the newly insured. Surely, this is not an acceptable reaction.Sadly, and for the wrong reasons, some of this may not come true, so some of the fears of the already-insured may be mitigated. Many states have indicated their plans to not participate in Medicaid expansion despite the financial incentives to do so (the federal government will pay 100% for the next several years, and 90% thereafter). These same states, as well as others, also pay so little under Medicaid that many doctors won’t see Medicaid patients. Unfortunately for that ignorant-or-selfish-or-both minority of seniors who say “keep the government’s hands off my Medicare!”, many of those same doctors are now refusing to accept Medicare patients. Hey, if they can make a big living without it, why should they take care of your mother? So if you are not on Medicaid OR Medicare maybe you’re safe – if you live in a relatively affluent part of an urban area, and have private insurance, and especially if you are in an integrated health system such as Kaiser that provides a strong primary care base.
The NYT article indicates that “Physician compensation is also an issue. The proportion of medical students choosing to enter primary care has declined in the past 15 years, as average earnings for primary care doctors and specialists, like orthopedic surgeons and radiologists, have diverged. A study by the Medical Group Management Association found that in 2010, primary care doctors made about $200,000 a year. Specialists often made twice as much.” In fact the gap is much greater than that between primary care physicians and specialists “like orthopedic surgeons and radiologists”; it can be several times greater. (This is because “specialists” includes, in addition, doctors like psychiatrists and some pediatric and medical subspecialists who earn much closer to what primary care doctors do, and thus bring down the “specialist” average.) A recent estimate was that an anesthesiologist can anticipate earning $7 million more in a career than a family physician!
I woke the other day to NPR to hear Republican senator Orrin Hatch saying “To be clear, it is a disgrace that so many American families go without health insurance coverage.” I was nearly ecstatic; to agree that something is a problem is the first step to getting together to solve it. And, surely, that something is “a disgrace” is even worse than being a problem. I turned up the radio to find out how Sen. Hatch and the Republicans were going to solve it. Unfortunately, that was not to be. It was a sound bite in a story by Julie Rovner titled “GOP Says Coverage For The Uninsured Is No Longer The Priority” (July 27, 2012). I hadn’t known it ever was a priority for the GOP, but this piece laid any doubts to rest. Worse than the double-talk from Hatch was Senate majority leader Mitch McConnell, in this excerpt:
McConnell: "Let me tell you what we're not going to do. We're not going to turn the American health care system into a Western European system. That is exactly what is at the heart of Obamacare. They want to have the federal government take over all of American health care."
By "Western European," McConnell means government-run or primarily government-run. Western European countries also pretty much don't have people who don't have health insurance. And by the way, there are closer to 50 million Americans without health insurance; 30 million is the number the health law is estimated likely to cover.
McConnell never says what the GOP is going to do, but you can be sure it will not have anything to do with covering everyone. This is too bad; there are possible solutions, and many of them are even based in the marketplace. Step one is for Medicare to completely revamp its reimbursement policies. This is because, to a large degree, Medicare reimbursement is the basis for all insurance reimbursement; while they may pay more (say, 1.5x Medicare) the ratios are the same, so if Medicare changes what it reimburses for primary care relative to subspecialty care, other insurers will follow.
In biological systems, the normal situation is to have “negative feedback loops.” For example, if the thyroid gland is producing enough thyroid hormone, it shuts down production in the pituitary gland of another hormone that stimulates the thyroid. When there is not enough thyroid hormone in the blood stream, the low levels stimulate the pituitary to become active, activating the thyroid gland. This is functional. Imagine how dysfunctional a “positive feedback loop” would be – the more the thyroid produced thyroid hormone, the more the pituitary would produce its stimulant, creating yet more thyroid hormone, and soon we’d all be hyper-thyroid and dead!
This is like the current medical reimbursement system. We pay doctors more to do procedures, pay them more to take care of only a few diagnoses in a limited organ system, pay them more if they live in an expensive area, and even more if they refuse to care for those on government insurance. This is a positive feedback loop where you economically do the best being a medical “partialist” in a nice suburban area taking care of relatively well-off people, and worst being a generalist in a rural area taking care of people who need it. Or, if you choose, work less than full time and still make a good living.
Medicare should immediately begin reimbursing primary care at a higher rate, including for the effort and cost of managing chronic disease, so that the income differential between generalists and specialists largely disappears. Then it should increase payments for doctors working in more rural and remote areas, not for “desirable” urban and suburban areas. Doctors practicing in urban underserved areas should get smaller incremental payments (after all, they can live in a “good” neighborhood and commute).
We will still have a shortage of doctors until the pipeline fills, but such a system will decrease the financial impetus to be yet another subspecialist in a metropolitan area that already has enough, and increase the impetus to become a generalist in an underserved area. If we are to depend on the market, this is the kind of market-based approach we need.